Coaching Clients on GLP-1 Medications: How to Protect Their Muscle While They Lose Weight
GLP-1 medications. Ozempic. Wegovy. Mounjaro. You've heard the names. Now you're seeing the clients. They're walking into personal training studios, booking consultations, and asking a question most coaches aren't fully prepared to answer: How do I make sure I'm losing fat, not muscle?
It's the right question. And it deserves a better answer than "eat more protein and do some weights." GLP-1 users face a specific physiological challenge that changes how you need to coach them. Understanding that challenge. and building a protocol around it. is one of the clearest opportunities in personal training right now.
What GLP-1 Medications Actually Do to the Body
GLP-1 receptor agonists work by mimicking a gut hormone that regulates insulin secretion and appetite. The clinical effect is powerful: appetite suppression in the range of 20 to 40 percent. Clients don't feel hungry. They eat less. They lose weight. That part sounds straightforward.
The problem is what they're not eating. When total caloric intake drops sharply, protein intake tends to drop proportionally. A client who was eating 150g of protein per day at 2,400 calories may drop to 60 to 80g per day once the medication kicks in. At that point, they're in a severe deficit with inadequate protein. That's not a fat loss environment. That's a muscle loss environment.
Research consistently shows that in the absence of resistance training and sufficient protein, roughly 25 to 40 percent of weight lost during caloric restriction can come from lean tissue. On GLP-1s, the caloric deficit is aggressive enough that this risk is elevated. Resistance training alone doesn't fully offset it if protein intake remains inadequate. Both levers need to be pulled simultaneously.
The Study Every GLP-1 Coach Should Know
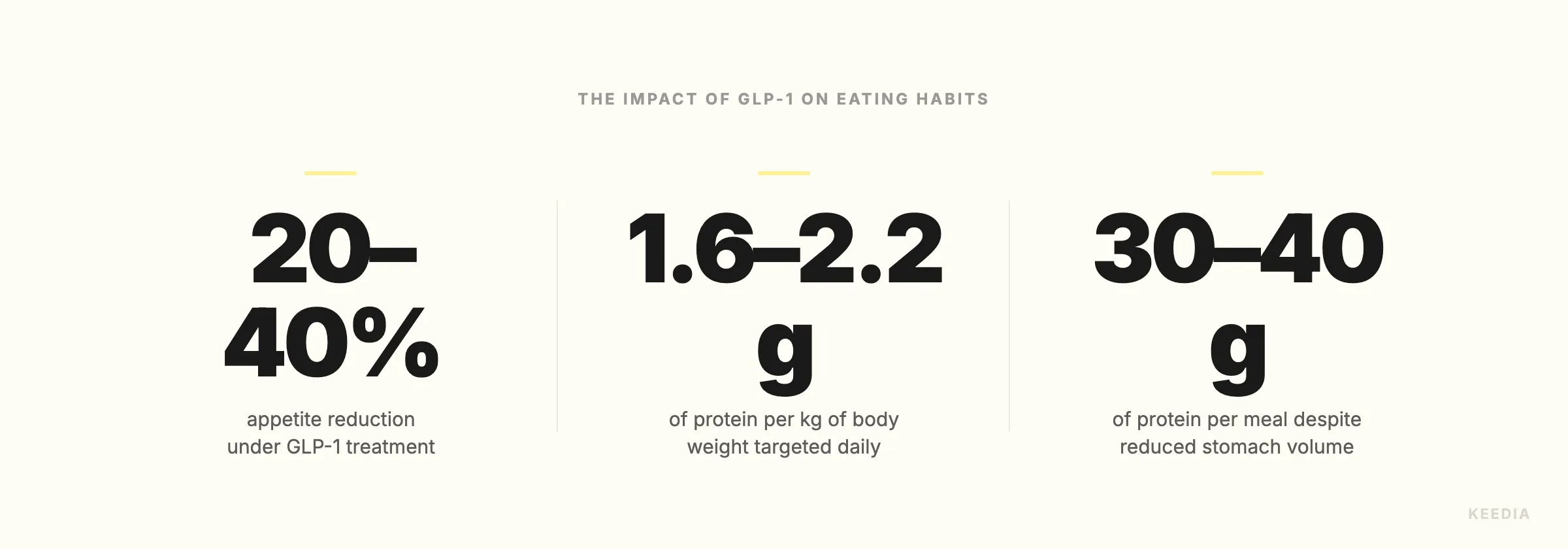
A 6-month study examining supervised resistance training combined with adequate protein intake in GLP-1 medication users produced results that should anchor every coaching conversation you have with this population. Participants who followed a structured protocol of 3 to 4 resistance training sessions per week, built around compound movements, lost nearly 24 pounds of fat. Muscle loss was kept under 1.5 pounds over the entire 6-month period.
That's a meaningful ratio. Nearly 24 pounds of fat gone. Less than 1.5 pounds of muscle lost. Compare that to what typically happens when GLP-1 users lose weight without a structured training and nutrition protocol, and you understand exactly what your value proposition is.
The training modality in that study wasn't cardio circuits or metabolic conditioning. It was structured, progressive resistance training centered on compound movements. That detail matters for how you build programs.
Rethink the Training Program From the Ground Up
The biggest mistake coaches make with GLP-1 clients is defaulting to the fat-loss playbook. HIIT circuits. Cardio-heavy sessions. High-rep, low-rest "metabolic" work. It's the wrong approach for this population, because the medication is already handling the caloric deficit. Your client doesn't need you to burn more calories. They need you to preserve what they're built.
Shift the training emphasis entirely toward muscle preservation and mechanical tension. The primary movements should be squats, deadlifts, hip hinges, horizontal and vertical presses, and rows. These are the movements that signal muscle retention at the systemic level. Accessory work can follow, but compound lifts should dominate session structure.
Program 3 to 4 sessions per week. Use progressive overload as the guiding principle, not caloric expenditure. Rep ranges in the 6 to 12 zone are appropriate for hypertrophy stimulus and are manageable for clients who may be eating less and recovering more slowly. Keep session length to 45 to 60 minutes. GLP-1 clients can experience fatigue and low energy on reduced intake, so volume management matters.
If cardiovascular training has a role, make it low-intensity and treat it as a recovery and cardiovascular health tool rather than a fat-burning strategy. Zone 2 training, done correctly, can support heart health and metabolic function without adding significant recovery demand. That's the appropriate framing.
Nutrition Coaching for GLP-1 Clients: Protein Density Per Bite
You're not a dietitian. But nutrition coaching within your scope of practice is essential with this population, and the core principle is simple: protein density per calorie per bite.
GLP-1 medications reduce stomach volume tolerance. Many clients report feeling full after two to three bites of a normal-sized meal. That means meals need to be small in volume but extremely concentrated in protein. The target should be 30 to 40g of protein per meal in as few calories as possible. Standard whole-food meals simply may not achieve this without strategic structuring.
Foods that work well in this context include Greek yogurt, cottage cheese, egg whites, white fish, shrimp, canned tuna or salmon, and lean poultry. Protein shakes can be useful as a supplement when clients simply cannot eat enough solid food in one sitting. The goal isn't to force volume. It's to prioritize protein within whatever volume the client can manage.
Encourage clients to eat protein first at every meal, before any carbohydrate or fat source. When appetite is limited and you can only eat a portion of what's on the plate, protein should be the portion that gets eaten. Coaching this behavioral habit consistently can be the difference between a client who retains muscle and one who doesn't.
Creatine monohydrate is worth discussing with GLP-1 clients as a well-supported supplement for muscle preservation, particularly during periods of reduced training capacity or illness. Understanding the differences between creatine forms helps you give clients informed guidance when they ask.
Managing Recovery on Reduced Intake
Recovery capacity changes when someone is eating significantly less. This is practical reality, not theory. GLP-1 clients may need more time between sessions, may experience greater soreness than expected, and may progress more slowly through strength adaptations than a client eating at maintenance or surplus.
Build this expectation into your onboarding process. Set honest timelines. Strength gains may be slower. That doesn't mean the program isn't working. It means you're managing the biology correctly.
Sleep quality and stress management matter more here than they do in a standard fat-loss program. If a client is consistently undersleeping or under significant psychological stress, muscle preservation becomes harder regardless of training and nutrition quality. Address these factors directly in your coaching conversations. The first 90 days are where most clients make or break their commitment, and GLP-1 clients dealing with medication side effects alongside a new training program need active support to stay engaged.
The Emerging Niche: GLP-1 Specialist Coaching
NESTA and ISSA have both launched GLP-1 Exercise Specialist certifications in 2025 and 2026. That's not a coincidence. When credentialing bodies formalize a specialty, it signals that market demand has crossed a threshold where a defined professional category is viable. This is where personal training is going.
The State of Personal Training in 2026 reflects a market that's segmenting rapidly. Generalist coaches are competing on price. Specialist coaches are competing on outcomes. GLP-1 coaching is a specialty where the demand exists, the supply of qualified coaches is limited, and clients are actively searching for help.
"GLP-1 fitness coach" is an emerging search term in both the US and UK markets. Clients who are spending $500 to $1,500 per month on medication are not price-sensitive when it comes to paying for a coach who understands what they're going through. They're solution-sensitive. They want someone who knows the protocol, understands the side effects, and can tell them exactly what to do.
If you're thinking about certifications, the investment in a GLP-1 specialization is modest relative to the positioning advantage it creates. Coaches who complete these certifications can credibly market themselves in a language that GLP-1 users are already using to search for help. That's a direct path to client acquisition without competing on price against generalists.
On the pricing side, GLP-1 specialist coaching justifies premium rates. If you're currently training clients at $80 to $120 per session, a documented specialty with a clear outcome focus supports rates in the $150 to $200 range. Pricing psychology shows that higher rates often improve client commitment and results, not just your revenue.
What a GLP-1 Coaching Protocol Looks Like in Practice
Here's a working framework you can adapt:
- Assessment: Track baseline body composition (DEXA or InBody if available, or circumference measurements as minimum). Establish protein intake baseline. Document medication dosage and any reported side effects.
- Training structure: 3 to 4 sessions per week. Compound-led. Progressive overload tracked session to session. Session duration capped at 60 minutes. Low-intensity cardio optional, framed as recovery support.
- Nutrition coaching: Protein target set at 0.7 to 1g per pound of bodyweight. Meals structured for protein density first. Protein supplement used if food intake is insufficient. Creatine discussed as a preservation tool.
- Recovery management: Sleep and stress addressed explicitly in check-ins. Deload weeks planned every 6 to 8 weeks, especially during periods of lower intake or high life stress.
- Progress tracking: Body composition reassessed every 4 to 6 weeks. Strength metrics tracked weekly. Protein intake logged and reviewed in check-ins.
- Communication: Weekly check-ins minimum. GLP-1 side effects (nausea, fatigue, reduced appetite) normalized and managed proactively. Referral relationship with a registered dietitian or the prescribing physician for questions outside coaching scope.
Why This Matters Beyond the Trend
GLP-1 medications are projected to be used by more than 30 million Americans by 2030. These are not fringe clients. They're your current clients, your future clients, and the clients your competitors haven't figured out how to serve yet.
The coaches who build competency in this area now. who understand the physiology, adapt their programming, and position themselves credibly in the market. are building a durable competitive advantage. The window for early positioning is open. It won't stay that way.
Your job isn't to manage the medication. It's to make sure the weight your client loses is the weight they actually want to lose. That's the brief. Build your protocol around it.