
Exercise as Effective as Antidepressants: What 2026 Research Found
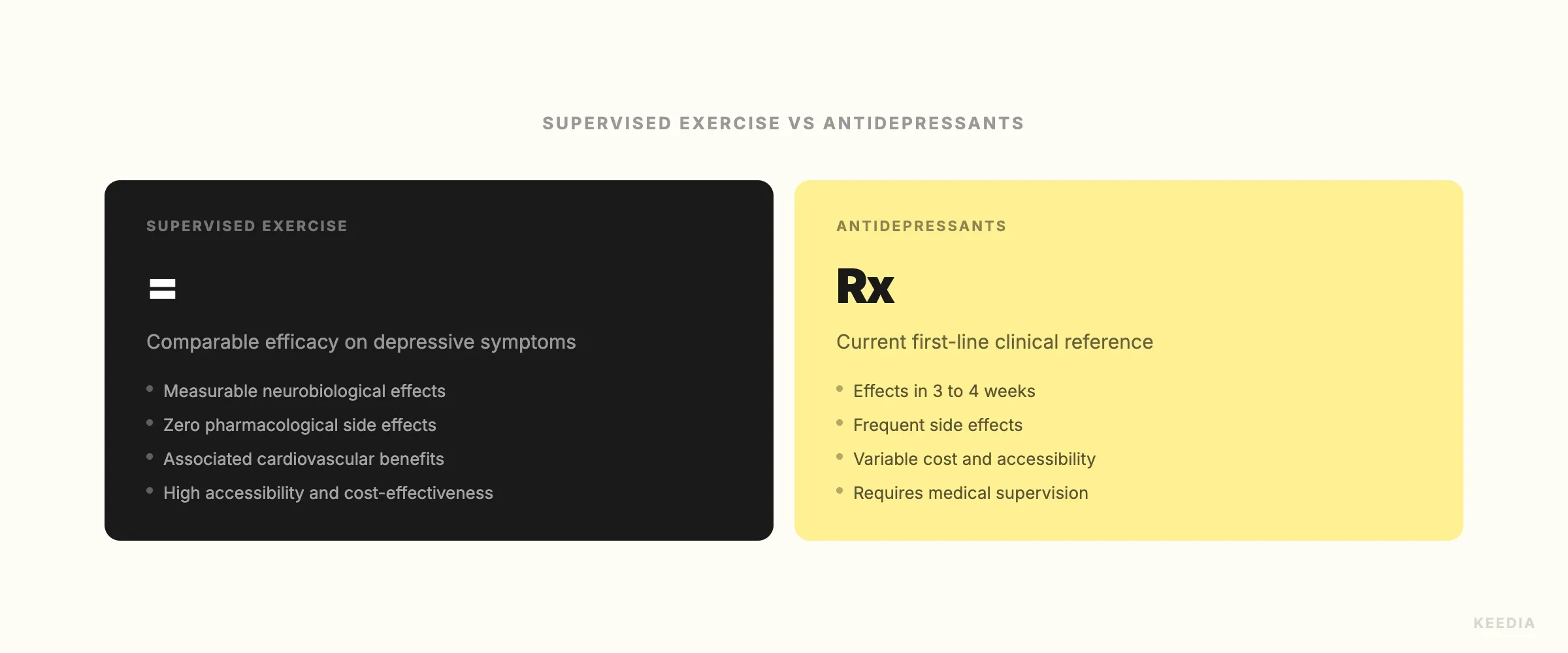
This isn't a motivational poster. A January 2026 meta-meta-analysis published in a major psychiatric journal reviewed hundreds of existing studies and reached a blunt conclusion: exercise reduces depression and anxiety symptoms at a level comparable to antidepressant medication and psychological therapies across all age groups. A concurrent large-scale randomized controlled trial confirmed the finding. NPR picked it up. The broader public started paying attention.
For anyone already training consistently, this reframes what you're doing. Your gym habit isn't just self-care or stress relief. It's a clinically validated intervention. And the specifics of how you train, and with whom, turn out to matter a great deal.
What the 2026 Research Actually Found
The January 2026 meta-meta-analysis synthesized data from dozens of prior meta-analyses, covering thousands of participants. Its scope was broad by design: it examined exercise interventions across adults of all ages, different clinical populations, and varied settings. The result was consistent across the board. Exercise reduced depressive symptoms with effect sizes comparable to first-line pharmacological treatments.
The concurrent RCT added controlled precision to the picture. Participants assigned to structured, supervised exercise programs showed statistically significant reductions in depression scores, on par with those in medication arms. Neither study argued that exercise should replace medication in every case. What they established is that exercise belongs in the same clinical conversation, not beneath it.
This is the distinction that matters for the fitness community. It's not that exercise is "good for your mood." It's that supervised exercise meets the evidentiary bar that medicine holds itself to.
Not All Exercise Is Equal: Why Supervision and Group Settings Matter
Here's where the research gets specific, and where fitness professionals should pay close attention. The largest antidepressant effects in the 2026 analysis were associated with aerobic exercise performed in supervised or group settings. Solo home training showed measurably weaker outcomes on mental health metrics.
That gap isn't surprising if you think about what group training actually delivers. You get structured progression, accountability, a coach monitoring your effort, and social connection. These aren't soft variables. They appear to amplify the neurological effects of the exercise itself.
The modalities with the strongest evidence include:
- Moderate-to-vigorous aerobic exercise (running, cycling, rowing) performed at least three times per week
- Group-based fitness classes with consistent attendance and social continuity
- Supervised resistance training, which showed meaningful but slightly lower effect sizes than aerobic work
- Combined aerobic and strength protocols in coached environments
If you're working with a coach or training in a group setting, you're already operating in the conditions that produce the strongest outcomes. If you're training alone at home, the data suggests you're leaving mental health benefits on the table, not because the movement is wrong, but because the context is incomplete.
The Mechanism: What's Happening in Your Brain and Body
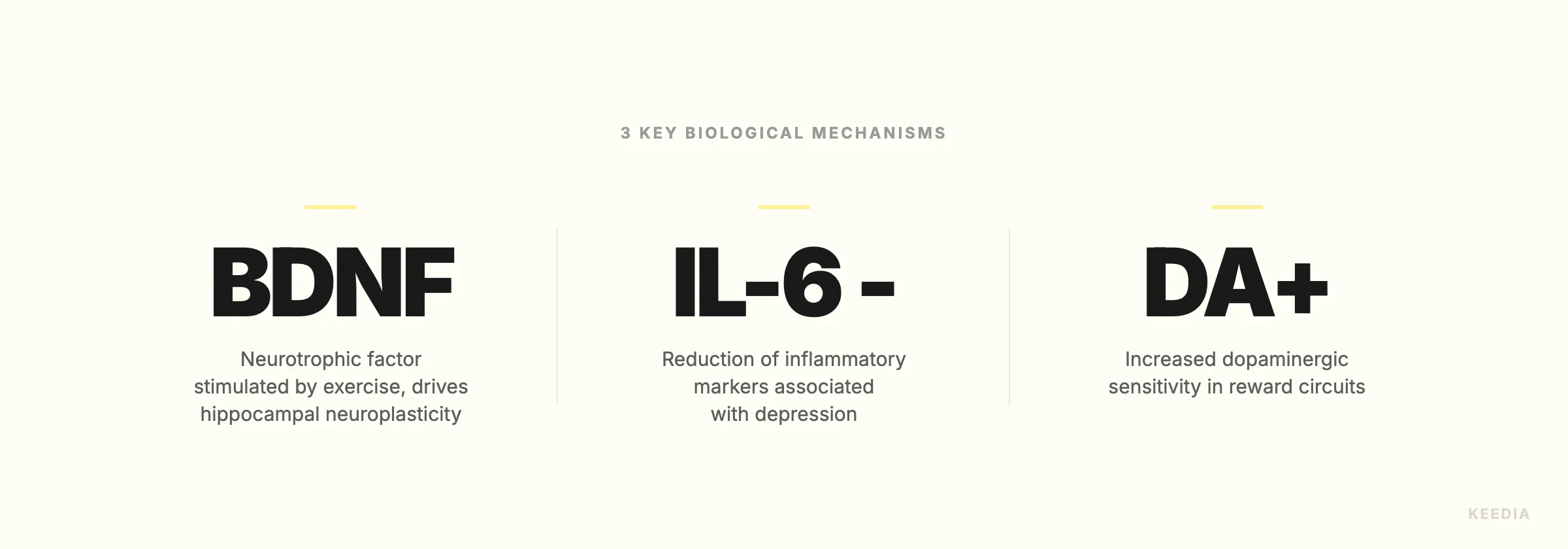
Understanding why exercise works at this level makes the results easier to trust and harder to dismiss. Three primary mechanisms are supported by consistent evidence.
Inflammation reduction. Chronic low-grade inflammation is increasingly recognized as a driver of depression, not just a side effect. Exercise, particularly aerobic training, reduces circulating inflammatory markers including C-reactive protein and interleukin-6 over time. This is one reason exercise appears effective even in treatment-resistant depression cases, where inflammation tends to be elevated.
Dopamine system restoration. Depression is often characterized by blunted dopamine signaling, which impairs motivation, reward processing, and anticipation. Aerobic exercise upregulates dopamine receptor sensitivity and increases dopamine turnover. This isn't a spike like caffeine. It's a structural improvement in how your reward circuitry functions.
BDNF and neuroplasticity. Brain-derived neurotrophic factor is a protein that supports the growth and maintenance of neurons. Exercise is one of the most reliable ways to increase BDNF levels in the brain, particularly in the hippocampus, a region consistently shown to shrink in people with chronic depression. Higher BDNF means greater neuroplasticity: the brain's ability to reorganize, adapt, and recover. Antidepressants also increase BDNF, which is part of why the two interventions produce comparable outcomes through overlapping biological pathways.
For context, this same neuroplasticity mechanism is relevant to cardiovascular health and cognitive performance. If you're interested in how aerobic capacity intersects with long-term brain and body health, how to improve your VO2max using research-backed protocols covers the training variables that drive the biggest adaptations.
Cost-Effectiveness and the Access Question
One of the most practically significant findings in the 2026 research is the cost-effectiveness argument. In the US, a standard course of antidepressant treatment combined with therapy can run $200 to $400 per month or more, depending on insurance coverage and provider access. A group fitness membership or semi-private coaching program often costs $100 to $250 per month. In rural areas or underserved communities where mental health providers are scarce, that gap is not abstract. It's the difference between access and no access.
The researchers explicitly noted that exercise should be considered a viable first-line intervention in populations with limited access to psychiatric care. That's a public health statement, not just a wellness recommendation. For gym owners, coaches, and fitness professionals, it's also a professional mandate. The environments you create and the access you provide carry clinical weight.
This matters for how coaches position their work. If you're a trainer who works with clients dealing with anxiety or low mood, you're not operating at the edges of your scope. You're delivering an evidence-supported intervention. Understanding what drives client churn at the 90-day mark becomes more relevant than ever when the stakes of consistency are this high.
Why the Gym Community Should Take This Seriously as Professional Evidence
NPR's coverage of the January 2026 findings in early 2026 signaled something worth noting. When research of this kind crosses over to mainstream media, the public conversation shifts. Physicians are increasingly likely to recommend structured exercise alongside or instead of medication for mild-to-moderate depression. That referral pathway runs directly toward gyms, coaches, and fitness programs.
The fitness industry has sometimes been reluctant to claim clinical territory, concerned about overstepping professional boundaries. That caution made sense when the evidence was thin. It makes less sense now. The research is peer-reviewed, replicated, and covered at scale. A supervised aerobic program delivered by a qualified coach in a group setting is, by the current evidence, a legitimate clinical tool.
This also connects to how fitness professionals talk about recovery, stress, and sleep. The same physiological systems that govern depression outcomes also govern adaptation, hormonal regulation, and sleep quality. For example, there's growing evidence that certain supplements support the recovery stack that makes consistent training sustainable. Magnesium's role in sleep quality for athletes, including which forms and doses produce measurable results, is part of the broader picture of how you support the nervous system that exercise is actively remodeling.
What This Means for How You Train
If you're reading this as someone who already trains, the implication is straightforward. Don't let your gym habit get reduced to aesthetics or performance metrics alone. The neurological and psychological benefits of consistent, supervised aerobic training are real, measurable, and clinically meaningful. They belong in how you think about your own health, and in how you talk about fitness to people around you.
If you're a fitness professional, this research strengthens your case in conversations with clients who are skeptical about gym membership costs, or who deprioritize training during periods of low mood, which is precisely when the evidence says they need it most.
The specifics to prioritize based on the current data:
- Aerobic exercise, three or more sessions per week, at moderate-to-vigorous intensity
- Supervised settings over solo training wherever possible
- Group formats that build continuity and social connection over time
- Consistent programming rather than sporadic high-effort periods
That last point is worth emphasizing. Consistency beats intensity for mental health outcomes. A sustainable training structure you follow for months outperforms a brutal block you abandon after three weeks. If you're thinking about how to structure long-term programming that holds up, research on cardiovascular health interventions and how to accurately identify your Zone 2 without lab equipment both inform the low-to-moderate aerobic work that the 2026 meta-analysis consistently flagged as most effective for mental health.
The science is no longer ambiguous. Exercise, done in the right context, works. Not as a supplement to real treatment. As one.