
GLP-1 Drugs Are Reshaping the Supplement Market — Here's What's Actually Growing
The rise of GLP-1 medications like semaglutide and tirzepatide isn't just a clinical story anymore. It's a consumer behavior story, a manufacturing story, and increasingly, a supplement industry story. According to NutritionInsight's 2026 trends report, GLP-1 drug adoption has "ignited change across the entire health ecosystem," with personalized supplementation emerging as one of the fastest-shifting sub-categories in the market right now.
For active people, whether you're on GLP-1 therapy or not, understanding what's actually driving this shift helps you separate legitimate product innovation from opportunistic relabeling. There's a lot of both happening simultaneously.
Why GLP-1 Users Create Specific Nutritional Gaps
GLP-1 receptor agonists work by suppressing appetite and slowing gastric emptying. That's the mechanism behind the weight loss. But it also means users are often eating significantly less food across the board, which creates predictable micronutrient gaps when intake isn't managed carefully.
The most commonly documented deficiencies in GLP-1 users include:
- Vitamin B12: Reduced consumption of animal protein, particularly red meat, cuts one of the most bioavailable dietary sources of B12. Long-term depletion affects nerve function and energy metabolism.
- Magnesium: GI motility changes, nausea, and altered food intake all suppress magnesium absorption. This matters across a wide range of physiological processes, from sleep quality to muscle function.
- Calcium: Reduced dairy consumption and lower overall caloric intake create a meaningful calcium gap, particularly relevant for women and older adults managing bone density.
- Iron: Lower red meat intake combined with potential GI irritation reduces both heme and non-heme iron absorption, increasing deficiency risk over months of therapy.
These aren't hypothetical risks. They're the same deficiency patterns seen in post-bariatric surgery populations, which GLP-1 therapy increasingly resembles in terms of metabolic effect. The supplement industry spotted this parallel early.
The Protein Problem Is Central
Of all the nutritional challenges GLP-1 users face, protein is arguably the most urgent. Reduced appetite translates directly into reduced total protein intake. At the same time, GLP-1 medications are associated with muscle loss alongside fat loss, a problem covered in depth in keedia's piece on GLP-1 and Muscle Loss: What Training Can — and Can't — Fix.
The compound effect is significant. You're eating less overall, so protein intake drops. But protein requirements arguably increase on GLP-1 therapy precisely because you need to preserve lean mass while in a substantial caloric deficit. Research consistently points toward 1.2 to 1.6 grams of protein per kilogram of body weight as the target range for people trying to retain muscle during weight loss, a target that's much harder to hit when appetite is blunted.
This is the legitimate driver behind the surge in protein supplement sales among GLP-1 users. High-quality protein powder, particularly whey and casein with complete amino acid profiles, solves a real problem here. It's a dense protein source that doesn't require a large meal to consume, which fits the reduced-appetite reality of GLP-1 therapy.
Protein supplement sales among adults over 40 have grown markedly since 2023, and market analysts attribute a meaningful portion of that growth directly to GLP-1 adoption in that demographic.
Electrolytes: A Pre-Existing Trend Gets a New Tailwind
Electrolyte products were already on a strong growth trajectory before GLP-1 drugs entered mainstream use. Sports nutrition data shows electrolyte sales up approximately 29% in recent years, driven largely by endurance athletes and the broader fitness community moving away from sugar-heavy sports drinks toward cleaner sodium, potassium, and magnesium formulations.
GLP-1 therapy is now adding a second demand driver. Nausea and vomiting are among the most common early side effects of semaglutide and tirzepatide, particularly in the dose-escalation phase that typically spans the first three to six months of treatment. Users who are vomiting regularly or experiencing significant GI distress face genuine hydration and electrolyte challenges that overlap directly with what endurance athletes manage during heavy training blocks.
The result is that electrolyte brands are marketing to two distinct audiences simultaneously, often with the same core product. For active GLP-1 users, this overlap is actually useful. The electrolyte formulations designed for athletic performance, adequate sodium, potassium, and magnesium without excessive sugar, are precisely what the clinical situation calls for.
Magnesium specifically deserves attention here. Beyond electrolyte replenishment, magnesium plays a documented role in sleep quality and recovery, something active people on GLP-1 therapy need to prioritize even more carefully. Keedia's breakdown of Magnesium and Sleep for Athletes: Which Form, What Dose, What Results is a useful reference if you're evaluating which form of magnesium actually does the work.
The "GLP-1 Companion" Marketing Explosion
Here's where you need to apply critical judgment. "GLP-1 companion" has become the fastest-growing supplement marketing claim of 2026. Walk through any major supplement retailer's website and you'll find dedicated sections for GLP-1 support stacks, GLP-1 companion bundles, and products positioned as essential co-therapy.
The reality is more mundane. The vast majority of these products are repackaged versions of existing supplements. A "GLP-1 support formula" is often a multivitamin with added B12, magnesium, and protein powder blended in, sold at a significant premium over buying those components individually. The nutritional logic is sound. The pricing frequently isn't.
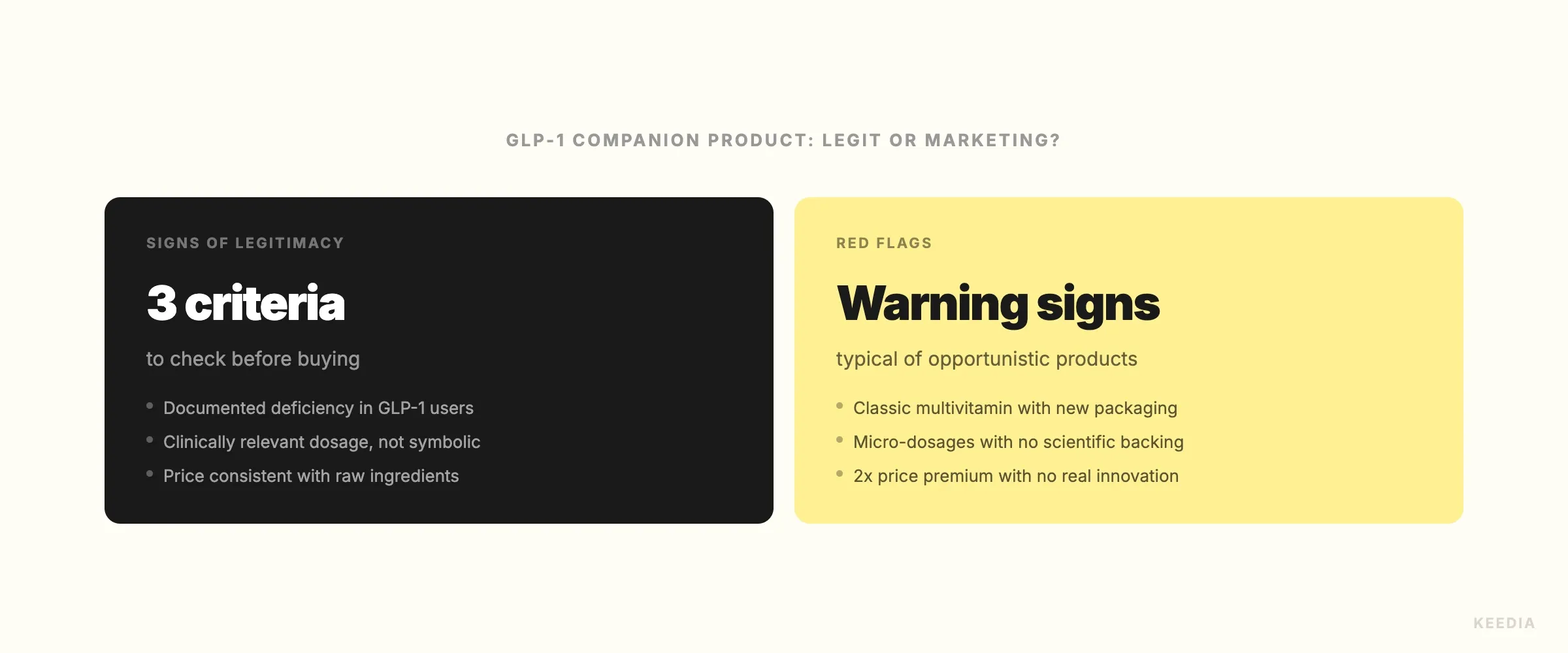
A useful framework for evaluating these products:
- Does it address a documented deficiency risk? B12, magnesium, calcium, iron, and protein are legitimate. "Metabolic support blends" with proprietary ingredients are not.
- Is the ingredient form appropriate? Magnesium glycinate and magnesium malate have better absorption than magnesium oxide. Methylcobalamin is better utilized than cyanocobalamin for B12. Form matters and should be listed clearly.
- Can you replicate it for less? In most cases, buying individual components from established brands costs significantly less than a bundled "GLP-1 companion" product. Compare unit economics before buying.
- Is there third-party testing? NSF Certified for Sport, Informed Sport, or USP verification matters for any supplement. GLP-1 companion branding doesn't change that standard.
Some brands are doing this legitimately, working with dietitians to formulate products specifically around GLP-1 deficiency profiles and pricing them competitively. Those products exist. They're just not the majority of what's flooding the market right now.
What This Means If You're Not on GLP-1 Therapy
The GLP-1 supplement wave has a secondary effect that's underreported: it's driving manufacturing scale in categories that benefit all supplement users.
When demand for high-quality protein powder, magnesium glycinate, and electrolyte formulations increases significantly across a market, manufacturers scale production. Larger production runs reduce per-unit cost. That cost reduction eventually passes downstream to retail pricing. You're already seeing this in the electrolyte category, where competition has intensified and price-per-serving on quality products has dropped over the past 18 months.
The same dynamic is unfolding in magnesium and B12 supplements, categories that were already growing but are now receiving disproportionate investment and competition. For active people optimizing nutrition without GLP-1 therapy, this means better product quality and lower prices across categories that are directly relevant to training and recovery.
Creatine is adjacent to this conversation worth noting separately. As GLP-1 users increasingly turn to resistance training and muscle-preservation protocols, creatine monohydrate is frequently recommended. If you're sorting through the noise on which form makes sense, keedia's comparison of Creatine Forms: Monohydrate vs HCl vs Buffered cuts through the marketing clearly.
The Broader Ecosystem Shift
GLP-1 drugs have created a new consumer archetype in the health space: the medically-assisted weight loss patient who is simultaneously trying to optimize fitness outcomes, preserve muscle, and manage side effects. This person is often highly motivated, health-literate, and willing to spend on supplementation. That's a valuable consumer for brands to target.
The supplement industry's response, predictably, is a mix of genuine innovation and aggressive opportunism. Separating the two requires the same critical framework you'd apply to any supplement category: documented need, appropriate ingredients, transparent labeling, and third-party verification.
The categories that are genuinely growing because of real demand are protein, electrolytes, magnesium, and B12. The categories growing primarily because of marketing are everything labeled "GLP-1 companion" that doesn't transparently disclose what's actually inside.
If you're active and navigating this market, whether on GLP-1 therapy or not, the fundamentals haven't changed. Eat enough protein. Cover your micronutrient bases. Choose supplements with verified ingredient quality. The new labels don't change the underlying biochemistry.