
Marathon des Sables 2026: What Actually Happens to Your Body During 252km in the Sahara
Right now, somewhere in the Moroccan Sahara, runners are carrying everything they need to survive on their backs and moving through one of the most hostile environments on earth. The Marathon des Sables 2026 runs April 3 to 13. Six stages. 252.8 kilometers. Daytime temperatures that routinely exceed 40°C in the shade. It's not a race you prepare for lightly, and it's not one your body forgets quickly.
This isn't a training guide. What follows is a breakdown of the extreme physiology happening inside every runner's body during those six days. The heat stress, the metabolic shifts, the sodium crisis that catches more athletes off guard than dehydration does, and why your feet take longer to recover than your lungs.
The Scale of What's Actually Happening Out There
The race is structured across six stages, with a rest day built in after the longest. Stage four, known as "the long one," covers roughly 85 kilometers in a single push. That's longer than two back-to-back marathons. Most competitors walk significant portions of it through the night, headtorches on, navigating dunes in the dark.
Runners are self-sufficient for food and equipment. They carry a mandatory minimum kit including sleeping gear, food rations, emergency supplies, and a compass. Race organization provides water checkpoints with a minimum of 1.5 liters issued per section. That figure isn't generous. It's the physiological floor.
The brutality here isn't just distance. It's the compounding of days. Each morning, your body starts in a deeper deficit than the one before. By day three, the physiology changes significantly.

Heat Is the Primary Physiological Enemy
During sustained effort in the Sahara, core body temperature climbs fast. Research on athletes in similar desert ultras shows core temperatures reaching 39 to 40°C during peak exertion. That's the threshold where cognitive function begins to decline, coordination degrades, and heat exhaustion becomes a real risk rather than an abstract one.
Sweat rates in these conditions exceed 2 liters per hour. Your plasma volume drops, cardiac output has to increase to maintain blood pressure, and the cardiovascular system is essentially running two jobs at once: delivering oxygen to working muscles and shunting blood to the skin for cooling. Something eventually has to give.
The body does adapt over repeated days of heat exposure. Plasma volume expands, sweat onset occurs earlier, and sweat becomes more dilute as the kidneys retain sodium more efficiently. This is the physiology behind structured heat acclimatization protocols, which research shows can improve performance in hot conditions by 4 to 8 percent when done over 10 to 14 days. If you're interested in how runners apply this before events like MDS, heat training for runners: protocol and performance gains covers the evidence base in detail.
But even well-acclimatized athletes face serious heat stress at MDS. The race provides mandatory medical checks, and withdrawal for heat-related illness is common. What surprises most people is what medical staff report seeing more often than heat stroke.
The Sodium Problem Nobody Talks About Enough
Hyponatremia. It's a drop in blood sodium concentration below 135 mmol/L, and it's caused not by dehydration but by drinking too much plain water. Race medics at MDS have documented hyponatremia as one of the leading causes of medical withdrawal in recent editions, occurring more frequently than heat stroke in some years.
Here's why it happens. You're sweating heavily, losing both water and electrolytes. You feel thirsty, which is correct. But if you replace that fluid with plain water at a higher rate than your body is losing it, you dilute the sodium in your bloodstream. The result is swelling in the brain. Symptoms include nausea, confusion, headache, and in severe cases, seizures. It mimics exhaustion so closely that athletes often don't recognize what's happening until it's serious.
The race issues salt tablets for exactly this reason. The mandatory 1.5L water minimum per checkpoint is designed to prevent dehydration without encouraging over-drinking. Electrolyte supplementation isn't optional at this scale of effort. It's the difference between finishing and a medical tent.
How Your Metabolism Shifts Over Six Days
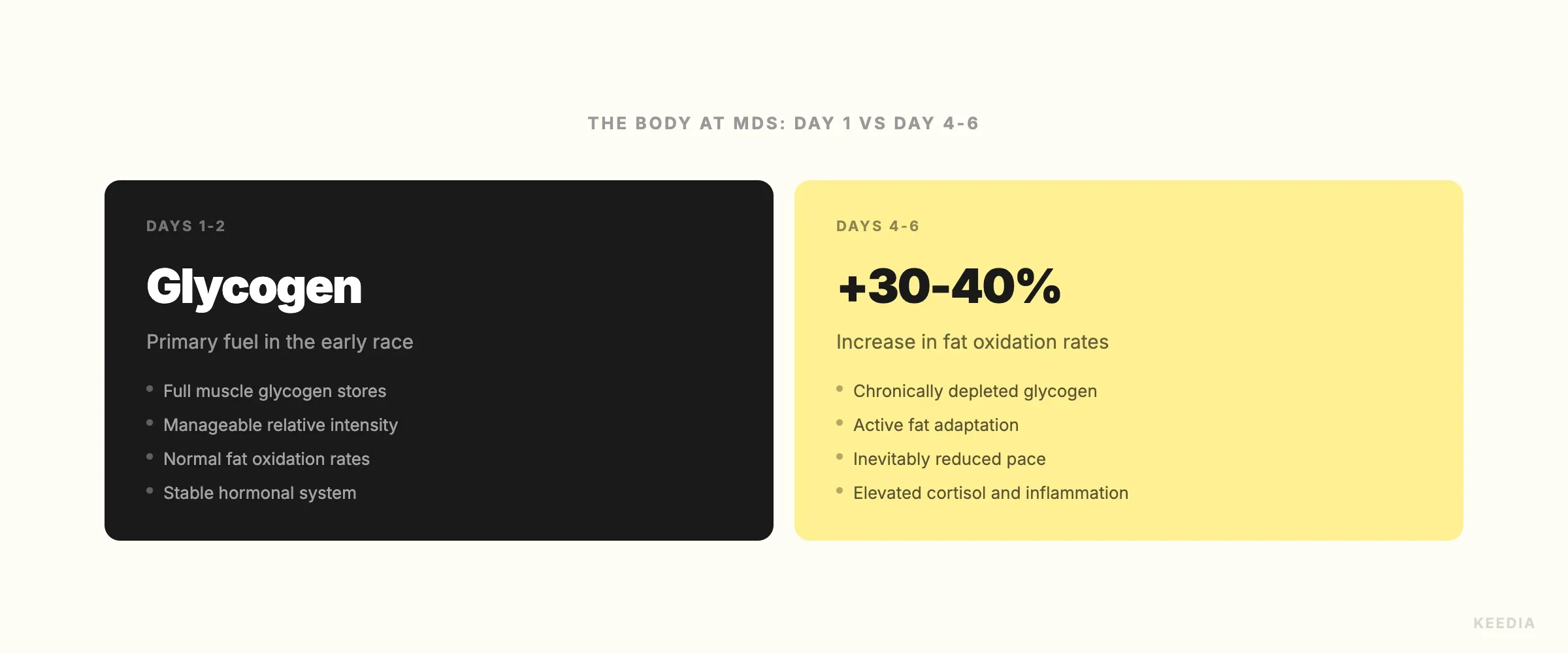
Day one, your body runs largely on carbohydrates. Glycogen stores in the muscles and liver supply fast energy for the effort. By the end of day two, those stores are chronically depleted. There's no full overnight refill when you're eating 2,000 calories from a pack you carried in. The body has no choice but to shift metabolic strategy.
By day three, fat oxidation becomes the dominant fuel pathway at intensities that would normally require carbohydrate. Research on multi-day ultra events shows average fat oxidation rates increase by 30 to 40 percent in the race's second half compared to early stages. The metabolic crossover point, where fat becomes primary fuel, shifts to higher intensities than it would in a rested, glycogen-replete athlete.
This isn't automatic. It's a forced adaptation, and it comes with a performance cost. Pace slows, perceived effort rises, and decision-making becomes harder as glucose availability to the brain decreases. Runners who carry higher-fat, lower-carb rations and have trained their fat metabolism specifically tend to handle this transition better. But everyone goes through it.
This metabolic stress also places significant demands on muscle tissue. Cortisol rises, muscle protein breakdown increases, and without adequate protein intake, you start losing lean mass. This is one reason why race nutrition weight calculations are so critical. Saving 200 grams of pack weight by cutting protein is rarely worth what it costs by day four. The research on how muscle catabolism interacts with extreme caloric deficits shares some overlap with current discussions around GLP-1 and muscle loss: what training can and can't fix, particularly around protein's protective role under prolonged stress.
What the Sahara Does to Your Feet
Foot damage is the number one cause of abandonment at MDS. Not heat stroke. Not exhaustion. Feet.
The combination of fine Saharan sand, sustained moisture from sweat, repetitive micro-trauma across 252 kilometers, and constant shoe friction creates blistering conditions unlike anything in standard road or trail running. Studies on MDS participants suggest up to 80 percent of runners develop significant blisters during the race, with many requiring medical drainage at daily field clinics. The race employs a dedicated team of medical volunteers, many of them podiatrists, to manage this specific issue at scale.
Gaiter use to prevent sand entry reduces abrasion significantly, and pre-race gait analysis to identify hot spots can reduce blister incidence by an estimated 40 percent. That's meaningful in a race where a foot injury on day two means carrying it across four more stages. For a broader look at foot and lower limb injury risk in prolonged running events, trail running injuries: the 2025 data and prevention protocols that work pulls together the most current evidence.
Toenail loss is nearly universal. Subungual hematomas form under nails from repeated impact against the toe box over consecutive long days. Most runners lose between one and five toenails in the weeks following the race. It's considered unremarkable by MDS veterans.
What Recovery Actually Looks Like After MDS
Finishing the Marathon des Sables is a physiological event your body doesn't quietly move past. The recovery timeline is significantly longer than a single marathon or even a standard 100-kilometer ultra.
Research on extreme multi-day endurance events shows elevated cortisol and systemic inflammatory markers persisting for two to three weeks post-race. Immune function is suppressed during this window, making infections more likely. Muscle damage markers, including creatine kinase, remain elevated for over a week in many participants. Sleep quality is often disrupted even after returning home, partly due to cortisol dysregulation.
The practical recovery timeline before returning to structured training is six to eight weeks. That's not arbitrary caution. That's what the physiology requires. Runners who push back into hard training before inflammatory markers normalize increase their injury risk substantially. The principles behind planned recovery from extreme events align closely with what structured deload protocols: what the research actually says recommends after periods of high physiological stress.
Connective tissue repair, particularly in tendons and cartilage after the repeated loading across sand, takes longer than muscular recovery. If you're supplementing during recovery, the current evidence on collagen and joint health: what the 2025 research actually tells athletes is worth reviewing, particularly around timing relative to loading sessions.
Sleep becomes critical in the post-race window. The body does most of its hormonal and structural repair during deep sleep, and after six days of minimal rest in the desert, that debt is significant. Most MDS finishers report needing nine to ten hours per night for the first two weeks after returning.
The Body Is the Race
The Marathon des Sables isn't won by the fastest runner. It's survived by the ones whose bodies manage heat, sodium, fuel, and tissue damage most effectively across six consecutive days. The dunes are the backdrop. The physiology is the actual competition.
Every runner out there right now is running a second race entirely inside their own biology. And that race doesn't end when they cross the finish line in Merzouga. It runs another six to eight weeks, quietly, in recovery rooms, compression socks, and a lot of extra sleep.